

- GENERAL SPONSOR
-

- SPONSOR
-

 |
|
NEWS & MOVIES ARCHIVE
Annual Scientific Meeting (EUBS 2009) in Aberdeen

The European Underwater and Baromedical Society Annual Scientific Meeting (EUBS 2009) were in King´s College,
We were there.
DIVING FOR HANDICAPPED PEOPLE IN THE WIDER ADRIATIC REGION
INTRODUCTION
Scuba diving use to be an activity available only to healthy and able-bodied individuals. Development of better diving equipment and systematic research concerning diving in the past thirty years made diving possible even for individuals with handicaps like asthma, amputation, diabetes mellitus, cerebral palsy, blindness, deafness, nerve and muscular disorders, sclerosis multiplex, spine injuries etc.1, 3 Scuba diving can help rehabilitation and become a recreational activity for people with handicaps.1, 3
Leading international organizations, which promote diving for handicaps, are Handicapped Scuba Association (HSA) and International Association for Handicapped Divers (IAHD).3 They take care about promotion of diving for disabled through teaching able bodied how to assist disabled divers. In the International Societies Association IAHD Adriatic we would like to take diving of handicapped divers to another level and enable handicapped divers even to become instructors for other disabled divers with minimum assistance of able bodied divers.
However, to keep it safe, training and diving of handicapped divers require special considerations. In 2002 we have developed a special project in
Eventually in 2006, we have established the International Societies Association IAHD Adriatic with founding organizations from
PROJECT DESCRIPTION
The project Diving for people with handicap started in
The program »Diving as a part of rehabilitation« is actually using diving as a therapy and it is created for individuals at the beginning of the rehabilitation process and also for individuals with various kinds of mental disturbances. The purpose of this program is not to train divers but to provide patients with an additional motivation for their active participation in rehabilitation process even if their limitations and handicaps are considerable. It is carried out in swimming pools. Trainees benefit of all the positive effects of hydrotherapy, such as easier and more independent movement, gaining a higher level of fitness, strengthening of different muscle groups and sometimes even easing the pain, spasticity and painful muscle spasms. With time, few of the trainees acquire some basic skills and wish for more. This program is now in its fifth year and includes protégés of day care centre Cebela and individuals after SCI from Institute for Rehabilitation of Republic of Slovenia. The age of participants vary from 28 to 62 years and their handicaps include Down syndrome, cerebral palsy, autism, traumatic head injury, blindness and spinal cord injuries.
The program »Diving through recreation« has been developing since 2002. It provides to handicapped individual a year around opportunity for recreation in the swimming pool with assistance of dive trainers which are also disabled. For those who are interested in becoming recreational divers program provides a formal diving course lead by divers with disabilities and their able bodied assistants. For disabled individuals we created standards which are based on C.M.A.S. minimum standards and requirements for recreational divers and instructors. We are taking special care about practical and theoretical education of able bodied assistants (divers and instructors). Our basic rule is that with diver with SCI there must be always two able bodied assistants for the sake of assistants’ own safety.
After seven years of systematic work we have acquired a significant experience in training and diving with recreational divers with SCI. There were no rules how to train them in environment where we live. We have been learning together ever since we started and our understanding of issues is rapidly changing. Today we know that thermoregulation is not that big hindrance for diving of paraplegics and quadriplegics. We do not spend months in the swimming pool with water temperature between 32 –
There are no special requirements for joining the course except that individual with SCI should be totally independent. Anyone who drives a car can become a certified recreational diver. The individuals with SCI have to take care about equipment (except SCUBA unit) and they have to be totally independent underwater. In the basic course (one star diver) we teach them proper techniques of arm swimming without use underwater propulsion vehicles (UPV). By passing the exam, which is the same as for all other recreational divers, trainee become certified recreational diver and may participate in organized diving holidays or dive in suitable diving centers. Until now, 25 divers have completed the education and 15 of them have been diving by themselves or through organized diving camps.
MONITORING SAFETY OF HANDICAPPED DIVERS
Although from the beginning of the program we have not registered any complications with the involved handicapped divers, safety of our trainees is our permanent concern. Due to the lack of specific studies pertaining to safety of handicapped scuba divers, we ask our trainees to dive conservatively and to document their experience. Collected data is sent for review to members of IAHD Adriatic advisory board (
In 2007 we did a field study at the
In cooperation with Medical School University of Split and Divers Alert Network we also conduct active monitoring of our graduates. The following is presentation of partial results of that effort.
METHODS
Dives for monitoring purpose is made individually or in a group of maximum five recreational divers with SCI. We asked divers to estimate their subjective perception of well-being and degree of fatigue before and after every single dive. They used ten-point scales, similar to the Visual Analogue Scale (VAS) for pain 4. On the scale of wellbeing the 1 means very unsatisfying state while on the other end the 10 signifies very satisfying state. On tiredness 10-point scale, 1 means very tired while 10 means not tired at all. We asked divers also to describe any medical problems they may have encountered during or after their dives. Information regarding the dive exposure (depth, duration, water temperature) was recorded by dive computers.
RESULTS
So far, the group of two female and thirteen male with SCI participated in gathering data. They were 27 to 49 years old. Their levels of SCI were from L1 to C6. They all were otherwise healthy. Some had a history of past uroinfections and decubital ulcers. None was taking any prescription drugs regularly. One was a diver before and got his spinal cord injury from decompression sickness 20 years ago. In the group of fifteen there were four smokers’, two males and two females.
Total 183 dives of divers with SCI were recorded from 2006 till now but in some cases documentation was not complete. Almost all dives were made in the
Results for 88 dives made by seven recreational divers with SCI (one female, six male), for which we gathered wider complete data showed that divers for perception of wellbeing before dive chose grades 7 or more in 94 % and after the dive in 81 %.
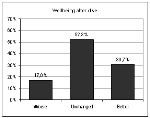
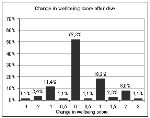
Figure 1 Figure 2
The estimation of wellbeing is shown in Figure 1 and Figure 2. The grade before and after diving was same in more than 52 %, better in 31 % worse in 17 %. When diver felt worse it was mostly for one point and mainly due to the cold. The worst result was reported by a subject who completed evaluation for 12 dives and felt worse after 6 dives. Four point negative score was recorded by same subject after repetitive dive because of dizziness.
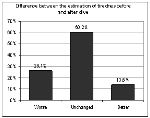
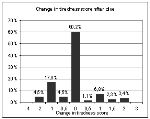
Figure 3 Figure 4
Tiredness before and after dive is shown in Figure 3 and Figure 4. Divers chose grades 7 or more before dive in 92 % and after dive in 89 %. In more than 60 % of the dives there was no difference in the assessment of tiredness before and after dive. In 14 % they were less tired after dive and in 26 % they were more tired after dive, but mostly for only one point. The greatest change in tiredness score was again reported by the same subject who was more tired after 50 % of dives.
Nobody reported any medical complications. One diver noticed that his urine almost regularly after dive became clearer what could be attributed to increased diuresis. One diver noticed that his spasms were less pronounced after dive and another noticed that the edema of the distal part of his legs shrunk.
DISCUSSION
Our results indicate that individuals with SCI find diving as a recreational activity suitable, interesting, and not at all straining. SCI divers swim with their arms and if they do not practice regularly they may not be prepared for long term swimming. Maintenance of physical fitness is even more important for SCI divers than for able-bodied. In absence of practice their swimming technique may degrade fast.
Immediate effects of diving were minor and mainly beneficial. However, improved health and quality of life SCI divers report since they assume diving could be attributable to hydrotherapy, regular physical activity, improved social interactions and psychological benefits of achievements and active life.
In spite of the fact that until now participating divers did not have medical complications, we believe that vigilance must be maintained. Data collection and documentation of experience of handicapped divers may increase our knowledge and contribute to dive safety for people with handicaps.
LITERATURE
1. Bove AA: Fitness to dive. In: Brubak AO, Neuman TS. Benett and Elliott`s Physiology and Medicine of Diving. 5th ed.
2. Breskovic T, Denoble P, Palada I , Obad A, Valic Z, Glavas D, Bakovic D and Dujic Z: Venous gas bubble formation and decompression risk after scuba diving in persons with chronic spinal cord injury and able-bodied controls. In: Spinal Cord (2008) 46, 743–747.
3. Degnan F: A guide for teaching scuba to divers with special needs.
4. Grabois M,
31. 08. 2009

















Production & design: Creativ, Novi mediji d.o.o.